
Let's be direct: no treatment cures baldness. What the best treatments do is slow or stop the underlying process — and in some cases partially reverse it. Here's the full landscape, sorted by strength of evidence, with honest assessments of what each option can and can't do.
Treatments With Strong Clinical Evidence
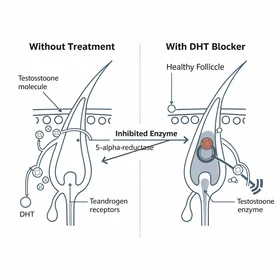
Finasteride (Prescription)
Finasteride inhibits Type 2 5-alpha-reductase, reducing scalp DHT by approximately 60%. It's the most extensively studied hair loss treatment, with Phase III trials showing 83% of users maintained or increased hair count over 2 years.
What it does well: Halts progression in most men. Produces measurable regrowth in many, particularly at the crown and vertex.
What it doesn't do: It's not a cure — hair loss resumes if you stop. Works better for crown than hairline. Sexual side effects (reduced libido, erectile dysfunction) affect 1–2% of users in clinical trials, with some reports of persistent effects.
Available as: Oral tablets (Propecia/generic), or topical formulations that reduce systemic exposure — such as Procerin Rx, which combines topical finasteride with minoxidil.
Minoxidil (OTC)
The most widely used over-the-counter treatment. Originally a blood pressure drug, minoxidil extends the hair growth phase and improves follicular blood supply. FDA-approved for hair loss since 1988.
What it does well: Proven efficacy for crown/vertex thinning. ~60% of men see measurable improvement. Available without prescription.
What it doesn't do: Doesn't address DHT — treats the symptom, not the cause. Hair regrown with minoxidil is lost within months of stopping. Less effective for hairline recession. Can cause scalp irritation.
Hair Transplant Surgery
FUE (Follicular Unit Extraction) and FUT (Follicular Unit Transplantation) relocate DHT-resistant follicles from the back of the scalp to balding areas. Results are permanent for transplanted hairs.
What it does well: Only option that permanently restores hair in bald areas. Natural-looking results with modern techniques.
What it doesn't do: Doesn't stop ongoing loss in non-transplanted follicles — most surgeons recommend continuing DHT-blocking treatment post-surgery. Expensive ($4,000–$15,000+). Limited by donor hair supply. Not appropriate for early-stage loss.
Treatments With Moderate Evidence
Natural DHT Blockers (OTC Supplements)
Saw palmetto, beta-sitosterol, pumpkin seed oil, and other natural compounds that inhibit 5-alpha-reductase at lower potency than finasteride. Available without prescription.
What the evidence shows: Several ingredients have small-to-moderate trial support. Saw palmetto showed statistically significant improvement in a head-to-head comparison with finasteride — though finasteride was more effective (66% vs. 38% improvement). Pumpkin seed oil showed 40% increase in hair count vs. placebo in a well-designed 2014 RCT.
Combination products that pair multiple DHT-blocking compounds with a topical component — such as Procerin — have shown results in IRB-approved studies. The combination approach (oral + topical) addresses DHT from both systemic and local pathways.
What they don't do: Natural DHT blockers don't match pharmaceutical-grade DHT suppression. They work best for early-stage loss and as a maintenance approach. Not a substitute for prescription treatment in advanced cases.
PRP (Platelet-Rich Plasma)
Concentrated platelets from your own blood are injected into the scalp. The growth factors are thought to stimulate follicle activity.
What the evidence shows: Several small studies show modest improvement in hair density. Evidence is growing but not yet definitive. Expensive ($500–$2,000 per session, multiple sessions needed). No standardized protocol — results vary significantly between practitioners.
Treatments That Don't Work (Despite Their Marketing)
This is where most of the hair loss industry's revenue comes from:
- Biotin supplements — Unless you have a documented biotin deficiency (rare), supplementation does nothing for androgenetic alopecia. The most overhyped ingredient in the hair loss space.
- Shampoos marketed as 'hair loss treatments' — The contact time of a shampoo on your scalp is measured in seconds. No active ingredient is meaningfully absorbed. Ketoconazole shampoo is the one exception — it has mild anti-androgenic properties when used regularly as an adjunct.
- Essential oils and scalp massages — No clinical evidence supports these for androgenetic alopecia. Some small studies on rosemary oil exist, but methodology is weak.
- Laser caps and combs — FDA-cleared (a low bar — it means 'probably safe,' not 'proven effective'). Evidence is limited and inconsistent. Expensive for uncertain benefit.
- Any product calling itself a 'cure' — If a product claims to cure baldness, it's either making an illegal health claim or it's not talking about androgenetic alopecia. Be skeptical.
The Realistic Approach

The most effective strategy for most men combines:
- A DHT-blocking component — pharmaceutical or natural, depending on your risk tolerance and stage of loss
- A growth-stimulating component — minoxidil or a topical activator
- Consistent, long-term use — months to see results, years to maintain them
- Realistic expectations — you're managing a condition, not curing a disease
Starting early matters more than which specific product you choose. A man who starts a basic DHT blocker at Norwood II will likely keep more hair than one who starts the most aggressive treatment at Norwood V.
For a more detailed look at treatment categories and how they compare, The Hair Loss Treatment covers each option in depth. For real user experiences with these treatments, Hair Loss Opinions collects and contextualizes actual feedback. And if regrowth is your primary goal, hair regrowth strategies focuses specifically on what's realistic at each stage.
Alternative Approaches to Baldness Treatment
No single treatment works for everyone, and understanding your alternatives helps you make a more informed decision. Here are the main options, with honest trade-offs for each:
- Finasteride (prescription) — the most potent pharmaceutical DHT blocker. Instead of natural supplements, some men opt for prescription-strength intervention. Trade-off: 1-2% risk of sexual side effects.
- Natural DHT blockers (e.g., Procerin) — saw palmetto and beta-sitosterol formulations offer a lower-risk alternative to pharmaceutical options. Less potent, but no reported sexual side effects.
- Minoxidil — a completely different mechanism (vasodilation) that can be used instead of or alongside DHT blockers. Better for crown thinning than hairline recession.
- Low-level laser therapy (LLLT) — another option for men who want to avoid both pharmaceuticals and supplements. Evidence is modest but growing. High upfront cost.
- PRP (platelet-rich plasma) — an alternative for men seeking a clinic-based approach. Expensive and requires multiple sessions, but avoids systemic medication.
- Hair transplant surgery — the only option that permanently restores hair in bald areas. Not an alternative to medical treatment but rather a complement — most surgeons recommend continuing DHT management post-transplant.
- Acceptance and cosmetic solutions — shaving, hair fibers, or scalp micropigmentation are legitimate alternatives for men who prefer not to pursue ongoing medical treatment.
The right choice depends on your stage of loss, risk tolerance, budget, and how much ongoing maintenance you're willing to commit to. Many men find the best results by combining two or more approaches — for example, a natural DHT blocker plus minoxidil.
Risks, Side Effects, and Safety Considerations

Every hair loss treatment carries trade-offs. Honest risk assessment is essential — ignoring the downside of any treatment leads to poor decisions and abandoned regimens. Here's what the clinical data shows about safety and limitations.
Finasteride Risks
The most significant side effects of oral finasteride include reduced libido (1.8% in clinical trials vs. 1.3% placebo), erectile dysfunction (1.3% vs. 0.7% placebo), and decreased ejaculate volume. These are generally reversible upon discontinuation. However, a subset of users report persistent sexual side effects after stopping — a phenomenon termed 'post-finasteride syndrome' (PFS). The risk of PFS remains debated: the Journal of Clinical Endocrinology & Metabolism (2012) documented cases, while Fertig et al., Journal of the American Academy of Dermatology (2017) found no statistically significant increase in persistent effects vs. placebo in a systematic review. Caution: women who are or may become pregnant should never handle crushed or broken finasteride tablets — the drug can cause birth defects in male fetuses.
Minoxidil Risks
Common side effects include scalp irritation, dryness, and flaking — particularly with the alcohol-based liquid formulation. The foam version reduces this risk. Less common effects include unwanted facial hair growth (from transfer) and, rarely, lightheadedness or rapid heartbeat. A safety note: minoxidil is toxic to cats, so pet owners should exercise caution with topical application.
Surgical Risks
Hair transplant surgery carries standard surgical risks: infection, scarring, numbness in donor/recipient areas, and the possibility of unnatural-looking results with an inexperienced surgeon. A specific limitation is 'shock loss' — temporary shedding of existing hair around the transplant site, which can be distressing even though it's usually temporary. The most significant long-term risk is progressive loss around transplanted areas if DHT management isn't maintained.
Natural Supplement Limitations
The primary limitation of natural DHT-management products is lower potency compared to pharmaceutical options. They may not provide sufficient DHT suppression for men with aggressive hair loss. The downside of saw palmetto specifically: a Cochrane Database of Systematic Reviews (2012) meta-analysis found the evidence 'limited and inconclusive' for benign prostatic hyperplasia, though newer hair-specific studies (Rossi et al., International Journal of Immunopathology and Pharmacology, 2012) showed more positive results when targeting scalp DHT.
Universal Warning
Consult a healthcare provider before starting any hair loss treatment — especially if you take other medications, have hormonal conditions, or have a history of depression or anxiety. DHT plays roles beyond hair follicles (prostate health, neurosteroid production), and modifying its levels requires medical oversight. This is particularly important for men under 25, whose hormonal profiles are still maturing.
No treatment is without risk. The goal is informed consent: understand the potential side effects, weigh them against the likely benefits for your specific situation, and make a decision with full knowledge of the trade-offs rather than marketing promises.
Cost is a real factor in choosing a treatment path, especially since most options require ongoing use. For a detailed breakdown of what each approach actually costs over 1 year and 5 years, see the hair loss treatment cost comparison.